69/F with shortness of Breath
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan. is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
A 69 years old female patient farmer by occupation came to casuality with chief complaints of SHORTNESS OF BREATH since 10 days
Decreased appetite since 4days
History of presenting illness::
Patient was apparently asymptomatic 5 years back then she developed Shortness of breath and was taken to private hospital was treated with Nebulization , Diagnosed as Bronchial Asthma and was on medication since then.
Shortness of breath seasonal variation ( every year during winters)
Patient developed similar complaints with fever and was admitted in Private hospital was treated as Bronchial asthma 6 months back
10days back she developed Shortness of breath grade MMRC grade 3 which was insidious in onset and gradually gradually progressive. Complaint of cough non productive, fever.
Not associated with chestpain , Palpitations, sweating
No history of orthopnea , paroxysmal nocturnal dyspnea.
Symptoms were relived in giving medication Nebulization
4 days back patient developed increased shortness of breath MMRC grade 4 , weakness , increased fatigue, decreased appetite, unable to move from bed or walk without support
Yesterday patient was taken to miryalaguda hospital with Complaint of shortness of breath and unable to swallow more for solids .
Evaluation was done and referred to our hospital
Past History:
10 years back patient had history of fall (head injury) which was not associated with loss of consciousness, projectile vomiting , seizure, weakness of limbs
Nueroimaging of brain was done
She was diagnosed with Hypertension and was started on medication.
Patient was diagnosed with hypothyroidism
since 4 years
Not a known case of DM, Tuberculosis ,epilepsy
Family History
Not significant
Personal History
Diet Vegetarian
Appetite Decreased
Sleep adequate
Bowel and bladder movements regular
No addictions and allergies to pollen dust
Daily routine:
She wakes up in morning
Eats 3 times
Walks around the house or sleeps
General Examination
Patient is conscious, coherent and cooperative
Well oriented to time place and person
Pallor -present

No Icterus, Clubbing, cyanosis,lymhadenopathy, pedal edema
Thin built and malnourshed

Vitals:
RR 27cpm
BP 110/70 mm Hg
PR 120bpm irregular
SpO2 89%on Room air and 96% on 2litres of O2
GRBS 141mg/dl
SYSTEMIC EXAMINATION:
RESPIRATORY SYSYTEM
Inspection
Shape of chest elliptical

Bilateral chest symmetrical
Equal chest expansion on both sides
Thoracoabdominal type
Trachea appears to be central
Supraclavicular hollow present
No muscle retraction, grunting, crowding of ribs
Palpation-:
All inspectory findings confirmed
No rise of temperature
No tenderness
Chest circumference 72 cm
Anterior posterior 20 cm
Transverse 32 cm
Ratio is 0.625 (5:8) (Normal is 5:7)
Trachea central
Symmetrical chest movements
Apex beat left 5th intercoastal space
Percussion-:
Resonant in all areas
Resonant in Right 6th Intercoastal space Tidal percussion
Auscultation-:
Bilateral air entry present
Crepitations at bilateral infra axillary area
Rhonchi at infra axillary and infra scapular area
CNS Examination
No focal nuerological deficiet.
CVS- :
S1 S2 heard, no murmur
P/A -
Soft, non Tender, no organomegaly
INVESTIGATIONS:
##COMPLETE BLOOD PICTURE::

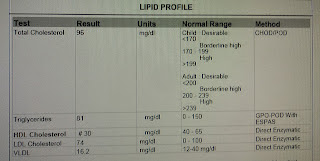
##LIPID PROFILE
##SERUM ELECTROLYTES

##ECG:

##SERUM CREATININE:



##Urinary electrolytes:

X RAY:



Asthama?
COPD ?
Miliary TB?
With Hyponatremia, hypokalemia


Comments
Post a Comment